Most specialty medical device companies plateau not because they've executed poorly, but because they're still running a commercial architecture designed for a stage they've already left.
The surgeon dinner went well. It always does.
A field rep wraps up a regional clinical meeting, flies home with a strong opportunity logged. The surgeon is engaged, vocal about wanting the device in his program, committed to championing it through value analysis next quarter. Six months later, the deal is still in play (technically). Biomedical engineering has questions about integration. Supply chain has a competing vendor on contract. The CFO is asking for ROI documentation in a format the company doesn't have. The surgeon is still trying, but he's stopped responding to the rep's check-ins. The deal is now twelve months out, optimistically. The rep gets pulled to an account where the cycle is further along. The surgeon's window, which was never as open as it looked, closes quietly.
This is not a deal running slow. This is a deal running exactly the way deals in this segment run.
The problem isn't the rep. The problem isn't the surgeon. The problem is that most specialty device companies at this stage haven't built a structural answer for how their commercial model has to change once they're operating here. What looks like a sales execution problem is, on inspection, something else entirely.
We've watched the following patterns appear, in some combination, in nearly every specialty device company we've worked with operating somewhere between $30M and $75M in revenue. They don't always appear in the same order but they almost always appear together.
The clinical champion who can't move the institution.
Surgeon advocacy gets you into the trial. It doesn't get you through Value Analysis. The translation gap between clinical preference and institutional adoption is where most opportunities stall. It's almost never the clinician's fault. The clinician was never the right person to translate the clinical case into the economic case the institution requires. That was never their job, and they were never equipped to do it.
The flagship-to-IDN expansion that never happens.
You win Memorial. Two years later, you still haven't won the parent system. The flagship win was driven by a single surgeon-champion relationship. System-wide standardization runs through procurement, biomedical engineering, finance, and executive sponsorship at the same time. No single relationship covers that map.
The KOL Advisory Board that calcified.
The same eight clinicians who validated the device at launch are still the Advisory Board four years later. They're brand-loyal. They're also no longer representative of the buyers you need to reach for the next chapter. The Advisory Board has become a relationship to maintain, not a commercial lever.
The territory you lost when the rep left.
A top-quartile rep departed. Their book of relationships left with them. The pipeline didn't transfer because it never lived anywhere except in their head. Eighteen months later, you're still rebuilding. The replacement is good, but they're starting from zero relationships and zero institutional memory on deals that were already in motion.
The senior commercial hire who couldn't move the curve.
You brought in a VP of Sales or Chief Commercial Officer with an excellent track record at a strategic acquirer or public medtech. Twelve months in, the trajectory hasn't shifted. The reason isn't the hire. It's that the playbook they're used to assumes infrastructure your company hasn't built yet. They arrived expecting to step into a system. There wasn't one.
The AI-enabled competitor on the shortlist.
A competitor added an algorithm and a regulatory pathway claim. They're now appearing in IDN evaluations you used to clear without competition. Your AI story is on the next board agenda. It isn't on the field team's deck. The gap is widening faster than the company is closing it.
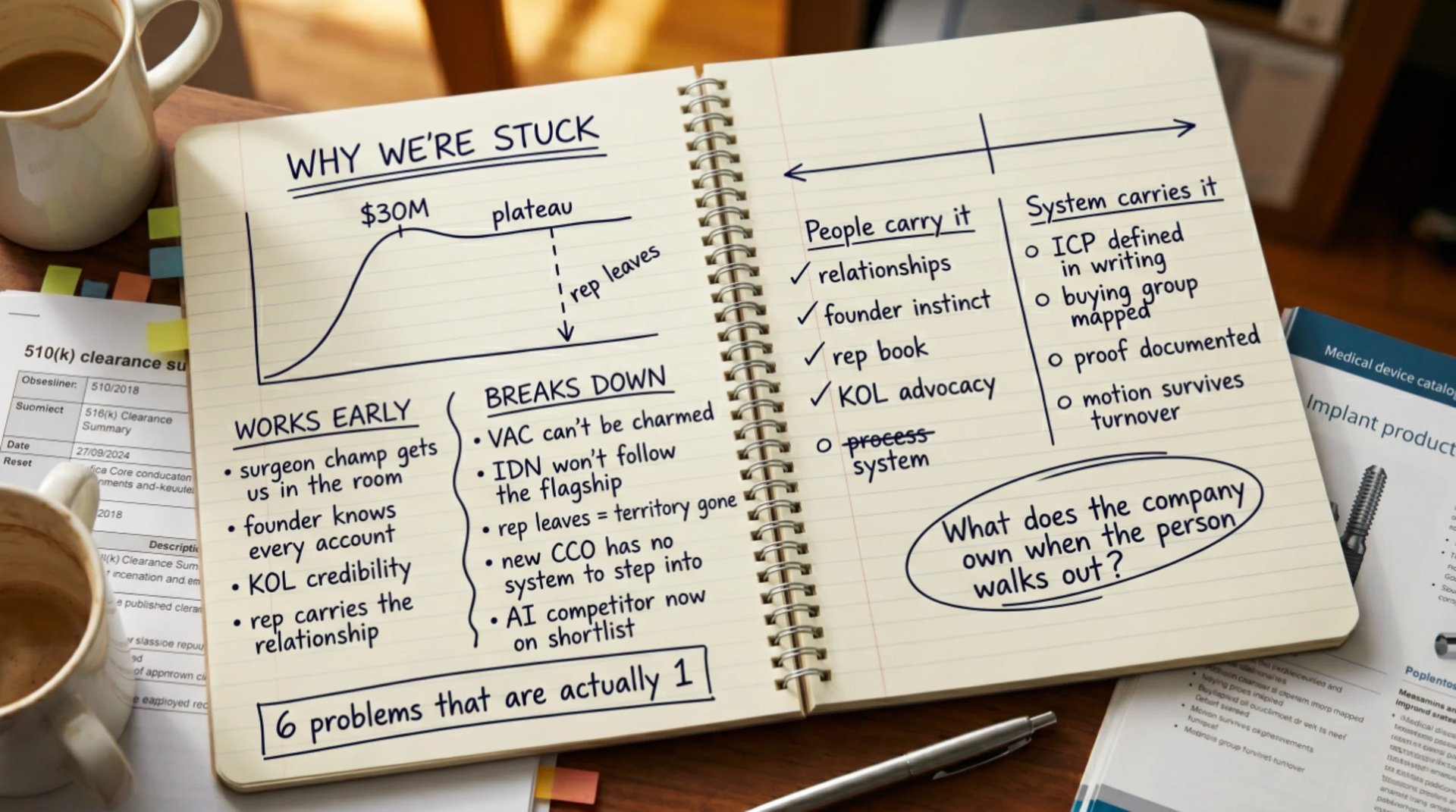
Most leadership teams treat these as six separate problems requiring six separate solutions. They hire a commercial leader for the rep dependency. An agency for the pipeline. A market access consultant for the IDN expansion. A workstream for the AI positioning story. Eighteen months later, the curve looks the same.
Assign each problem to a different owner. Sales fixes the rep dependency. Marketing fixes the pipeline. Business development owns the IDN expansion. The new CMO owns the AI narrative. This is a reasonable organizational instinct. It also doesn't work.
These aren't six problems. They're one problem, expressing itself in six places.
Every pattern above is what happens when a commercial growth model runs on people-based mechanics (surgeon-champion relationships, individual rep books, founder-driven sales motions, KOL advocacy) and asks those mechanics to do work they were never structurally designed to do at scale.
This is a specialty medtech pattern, not a generic B2B problem. Three structural reasons explain why.
Clinical credibility is people-based by necessity in the early chapter. You can't shortcut it. You need surgeon advocates to validate the device. This is correct for the stage. It also means the model the company builds is people-based from inception. The architecture that works at clearance and through the first 30 to 50 accounts is the same architecture that starts failing between $30M and $75M.
The capital purchase dynamic concentrates decisions in a small number of high-stakes meetings. Individual relationships become load-bearing in a way they don't in other B2B environments. A software company spreading 200 deals across a year can absorb relationship turnover. A specialty device company doing 30 capital placements cannot absorb it the same way.
An 18-month sales cycle compounds turnover risk in ways most industries don't face. Losing a champion or a rep midway through a deal is unusually costly here. The exposure is structural, not circumstantial.
The growth model that works for the first chapter of a specialty device company is a different model from the one required for the second. Companies that don't recognize this plateau between $30M and $75M. Which is where most of them are still sitting.
Most leadership teams at this stage have already tried to address some of these patterns. The question isn't whether the fixes were good-faith efforts. It's whether the kind of fix applied can address the underlying problem.
The senior commercial hire. The new VP or CCO arrives expecting a commercial system to step into. There isn't one. They spend their first nine months trying to build the system while being expected to hit the number at the same time. Most fail inside 14 months. The hire wasn't wrong. The substrate they were dropped into was.
The medtech-specialist marketing agency. Better-looking campaigns. They still reflect whatever positioning lives in the founder's head, because there's no documented strategic architecture for the agency to draw from. After 12 months, the company has new branding and the same growth curve.
The PE operating partner's playbook. Worked at the last three portfolio companies. Imported wholesale into a specialty device company at this stage, it creates friction. It assumes systems that aren't installed yet, and the company spends six months arguing about implementation instead of executing.
The strategy consulting engagement. Excellent diagnostic. Forty-page deck. The deck describes what should be true. It doesn't install what needs to be true. Six months later, the deck is in a drawer.
Each of these is a people-based intervention applied to a people-based system. They reinforce the architecture. What this stage of growth requires isn't another person added to the model. It's a different model.
A different model is the last thing anyone wants to hear. It implies the work already done was wrong. It wasn't. It was right for the stage it served. The question is whether it's right for the stage ahead.
The alternative isn't more strategy documents or another senior hire. It's an installed operating system that defines, in writing, in a form any rep or commercial leader can step into: who the company actually serves and who it doesn't, the full buying group for each target account with the right entry point per stakeholder, the differentiated outcome and the proof that lands credibly with clinical, technical, and financial buyers, and the commercial motion that doesn't have to be rebuilt every time a person turns over.
The practical difference looks like this:
In a people-based model, institutional knowledge of a buying group lives in one rep's head. When that rep leaves, it's gone.
In a system-based model, that knowledge lives in a documented architecture the next person inherits on day one. The deal doesn't restart. The territory doesn't reset.
This is what we call a Growth Operating System. Not a strategy deck. Not a playbook. An installed architecture that belongs to the company.
The point isn't sophistication. It's removing the dependency on any one person (the founder, the top rep, the surgeon-champion, the next senior hire) and making growth a function of the system rather than of the relationships.
If these patterns are familiar (and they usually are if your company is somewhere between $25M and $75M in specialty device revenue), the question isn't which one to fix first. They aren't separable. The question is whether your current growth model is the one that will carry you into the next chapter.
The first step isn't a new hire or a new agency. It's an honest look at how your current positioning is actually landing with the buyers you're trying to reach. The Market Perception Audit is designed for that: ten minutes, no conversation required, structured output you can use whether or not we ever talk again.
The reason nothing is changing isn't that you haven't tried hard enough. It's that you've been treating one structural problem as six separate ones. There's a different way to look at it. There's also a different way to fix it.
Ready to see where you stand?
If your company is between $25M and $75M in specialty device revenue and the patterns in this article sound familiar, the audit is where to start. No pitch. No prep required.
No commitment. No pitch. Structured output you can use the same day.
